The Successful Esthetic Rehabilitation Through Simulations

The most critical factor to communicate to the laboratory for managing control over an esthetic rehabilitation case is the dentofacial smile design. Imagine the predictable restorative success we all could attain in the esthetic zone if we provided the laboratory with the tooth arrangement and form; the ratio of tooth width to height; and illustrate how these relationships are perceived against the unique facial properties of each patient. If these metrics are truly what determines successful esthetic cases, then the burden to communicate those relationships to the ceramist would lie with the practitioner, without error.
The question then becomes how best to communicate these metrics? The most precise method of communicating intra-arch tooth position against the unique facial properties of the patient is through a series of digital simulations and corrections that are refined and mapped throughout the management of the case using a digital intraoral scanner.
If facially-driven form and tooth arrangement are the most important visual determinants of a successful esthetic rehabilitation case, our objective as practitioners is to find this relationship, then manage the patient’s bite forces and chewing patterns to fit within that design, or conversely, to adjust the design to fit within existing bite forces and chewing patterns of the patient. At our practice, we manage this by utilizing the Kois Management Considerations: The 10 Step Approach (see sidebar) to evaluate and adjust the dentofacial, functional, biomechanical and periodontal considerations within CAD software (Exocad) to create a series of simulations.
Digital simulations and direct mockups are utilized to determine optimal dentofacial form of the smile design. The objective is to refine each simulation in a step-by-step manner until the desired, harmonious relationship of the new smile design is realized. In our restorative routine, every case can be simulated four times within our workflow if necessary. Built first upon the Primary digital simulation, subsequent simulations are transferred directly to the patient and refined directly.
Primary Simulation
A full-face photo along with three close-up photos of the patient are taken: lips at rest, full smile; and retracted mode. The photo of the retracted patient in a neutral head position is imported into CAD software along with an initial intraoral scan (Trios-3, 3Shape) of the maxillary arch. The intraoral scan is matched in size and scale against the photo of the retracted patient (our digital facebow transfer).
Note: Click images to enlarge.

Figure 1. Initial Digital Scan
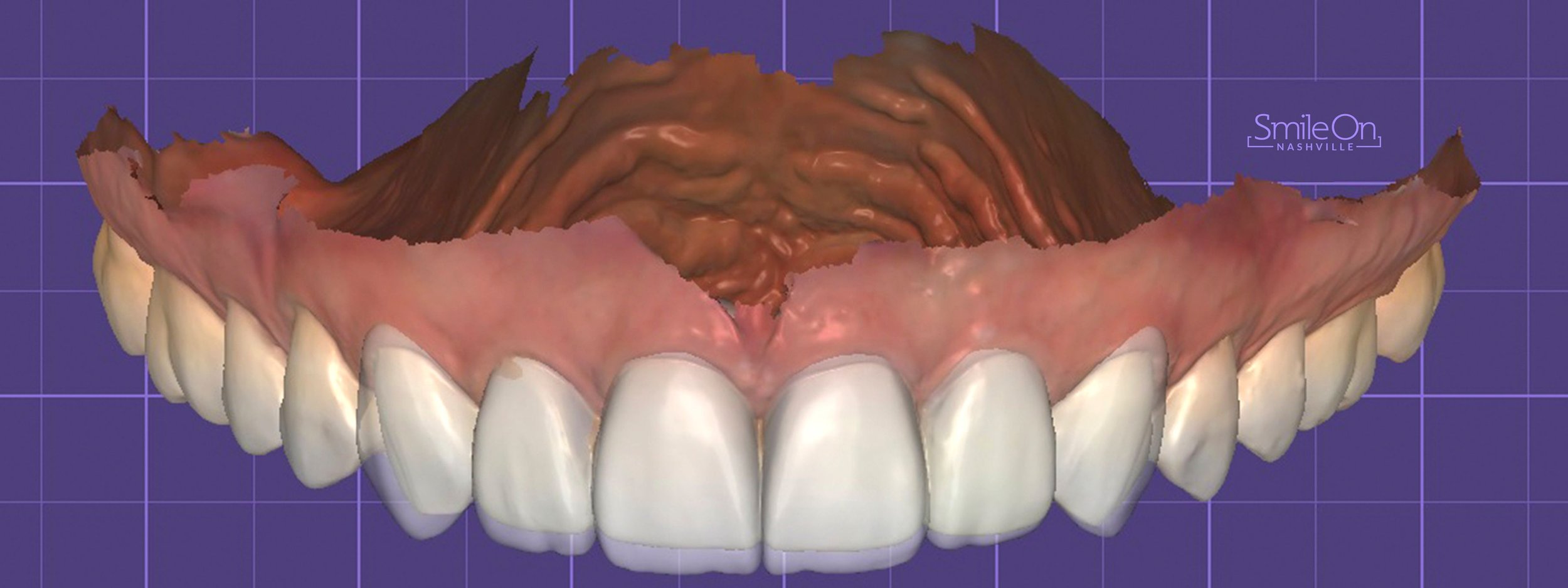
Figure 2. Primary Digital Simulation: proposed tissue adjustments to achieve a more aesthetic height/width ratio. Gingivectomy planned for teeth 6-11. Veneers planned for 6 & 11.

Figure 3. Primary Simulation. Before Treatment - Old Veneers
Figure 4. After - Final Restorations
A new design is created utilizing various tooth libraries (much like setting denture teeth in wax). The CAD software digital articulator functions allow us to create new dentofacial arrangements while honoring or adjusting bite forces and wear patterns. The objective of the Primary Simulation is to reconcile general tooth form, arrangement and positioning, relative to crown length and negative spaces in a completely additive manner to prepare for a direct transfer to the patient. This must be an additive or neutral step against the existing dentition. Once completed, models are 3D printed, washed and cured. A silicon index of the proposed smile design is created in preparation for direct transfer.
Note: The analytical, left-brained dentist, who strictly adheres to the golden ratio, may object to this method, while the artistic, right-brained dentist sees the value in an additive design simulation. However, by the secondary simulation, both left- and right-brained dentists will see the value of the additive Primary Simulation.
Secondary Simulation
Note: Click images to enlarge.

Figure 5. Secondary Simulation
In the Secondary Simulation direct application of the Primary Simulation is executed and adjustments are made. The Primary Simulation is applied to the patient using a silicon index and bisacryl resin. Excess bisacryl is trimmed using 7901 carbides where needed and interdental closure spaces deepened so the teeth appear separated once applied to the patient. At this point we capture photographs of the patient with the proposed design and allow the patient to review the design. Often, the Primary Simulation does not need to be altered and the patient is motivated to move forward.

Figure 6 Secondary Simulation
If design changes are desired, the focus turns to altering vertical proximal crests (transition lines between the proximal and facial), levels and volume of interdental contact points and length. These four adjustments are typically needed to size down or carve the Secondary Simulation. When configured properly, a digital impression scan is captured and refined in the CAD software (Exocad). Models are reprinted and a new silicon index created and prepared for the preparation appointment.
Note: The additive design placed directly over patients existing ceramics and canines utilizing putty stints and integrity bisacryl. Photographs captured and presented to patient for approval of new design.
Tertiary Simulation
At this point, the patient generally accepts the design, form, and morphology of the treatment proposal. Following tooth preparation, the silicon index is used to place the final temporaries. In this simulation, additive adjustments to the design are made with a composite material (Tetric Evo Ceram, Ivoclar Vivadent) to sharpen transitional line angles. Reflective and deflective surfaces are established with fluted carbine finishing burs and polishing disc (3M). Final photos and digital impressions are captured and sent to the laboratory. The ceramist is instructed to strictly adhere to the design.
Note: Click images to enlarge.

Figure 7. Preparation

Figure 8. Preparation

Figure 9. Preparation
Note: After removing existing ceramics 7-10, the over prepared anterior were cleaned with aluminum oxide air abrasion. Teeth 6 and 11 were minimally prepared to relocate incisal position and establish canine guidance.
On rare occasions, a patient is asked to return 1-2 days following the preparation appointment to evaluate the design without the effects of anesthesia. If adjustments are needed, which typically involves length or volume requests, the adjustments are completed, and the information is sent to partnering laboratory with digital photos.
Note: Click images to enlarge.

Figure 10. Tertiary Simulation

Figure 11. Tertiary Simulation

Figure 12. Tertiary Simulation

Figure 13. Tertiary Simulation
Note: Gingivectomy to balance tissue and tertiary simulation placed and contoured to patients approval. Notice the emphasis of canine incisal edge position and an increased height to width ratio of the centrals.
Key Information for Laboratory Communication
The laboratory should receive three scans and three photo series.
Scans: Initial scan, Preparation scan, Final Simulation
Photos: Initial photo, Polarized preparation photo and adjacent teeth with shade tab, Tertiary Simulation with notes for ceramist Final Simulation photo.
Note: Click images to enlarge.

Figure 14. Final

Figure 15. Final

Figure 16. Final

Figure 17. Final
Note: Cutback HT-BL2 IPS e.max veneers seated. Canine guidance established to protect lateral incisors during excursive movements. Macstudio Restorations by MicroDental Laboratories.
Upon receipt of the three digital scans, the laboratory syncs the models, using common soft tissue landmarks, and held in proper orientation based on the position of the initial scan, which is properly oriented from the digital face bow transfer of the head in a neutral position. Adjusting opacities of the scans allows the laboratory to see a precise relationship between the initial scan, the preparation scan and final simulation scan. At this point we have controlled the most important aspect of a successful rehabilitation in the esthetic zone: the dentofacial design. The ceramist is now tasked with characterizing, layering and enhancing the three-dimensional light properties of the ceramics.
A powerful implication of the simulation process is that once restorations are seated and scanned for a night guard, this fourth scan can be synchronized with the previous scans to evaluate the accuracy between the final simulation and the final restorations. The feedback loop from case to case will aid in predictability, cooperation and precision between the laboratory and practitioner.
*
Conclusion
Digital technologies have significantly changed the clinical approach to esthetic restorative dentistry and, using this 3-step protocol, can provide practitioners with the ability to efficiently exert more control over the restorative design and final execution of comprehensive restorative cases. Powerful chairside software applications along with proven clinical case management protocols now allow clinicians to control the morphology of the smile, incisal edge position and embrasures, line angles as well as reflective and deflective surfaces and offer the highly skilled ceramist the information needed to perform at the highest levels.
Sidebar
Kois Management Considerations - The 10 Step Approach
Develop Maxillary Incisal Edge Position
Develop Maxillary Posterior Occlusal Plane
Develop Mandibular Incisal Edge Position
Mandibular Posterior Occlusal Plane
Intra Arch Tooth Position
Gingival Tissue Assessment
Therapeutic Considerations
Restoration Design
Gingival management / control loss of attachment
Restoration enhancement / concerns
About the author:

Dr. Jeff Trembley
Dr. Trembley was raised in Knoxville, TN where he attended college as a pole vaulter for Tennessee’s Track and Field Team. An avid striper-fisherman and volleyball enthusiast, Trembley moved to Nashville from 2006–2008 to teach science at Montgomery Bell Academy in Nashville, TN. In 2009, Trembley was accepted into Dental College in Memphis, TN where he found his passion for dentistry. After 4 years of private practice in Middle Tennessee, Trembley opened Smile On Nashville in November 2017.